Introduction
Population aging is a global phenomenon, with South Korea experiencing one of the most rapid demographic shifts toward a super-aged society. This transition highlights a critical public health challenge: extending not just lifespan, but “healthspan,” ensuring that older adults can live independently with a high quality of life [1]. Central to healthy aging is the preservation of physical function, as its decline is a primary driver of frailty, disability, and increased healthcare dependency [2]. While functional decline in older adults is comprehensively assessed through various well-established measures, including gait speed, balance tests (e.g., the Timed Up and Go test), and multi-component batteries like the Short Physical Performance Battery (SPPB), these assessments often require trained personnel, specific equipment, and dedicated space, which can limit their application in broad, community-based settings. Therefore, identifying a more accessible, yet equally reliable, indicator is crucial for effective and widespread public health screening.
Among the available indicators, handgrip strength (HGS) has emerged as an exceptionally robust and clinically significant biomarker of overall health and vitality in older adults [3]. Its particular importance lies not only in its strong reflection of overall muscle strength but also in its unparalleled practicality. Unlike other functional tests, the measurement of HGS is simple, rapid, non-invasive, and highly cost-effective. This efficiency makes it an ideal tool for large-scale, opportunistic screening of functional status within busy primary care and community health settings, where time and resources are often constrained. A substantial body of evidence has established low HGS as a strong predictor of numerous adverse health outcomes, including sarcopenia, falls, increased morbidity, prolonged hospitalization, and all-cause mortality [4-6]. Consequently, HGS is no longer viewed merely as a measure of hand function but as a vital sign reflecting an individual's underlying physiological resilience [7].
The decline in HGS is influenced by a complex interplay of various factors. While the impact of non-modifiable factors like advancing age and sex is well-documented, a comprehensive understanding requires examining a broader set of determinants. For instance, physiological factors such as overall muscle mass are intrinsically linked to strength [8]. Additionally, socioeconomic conditions like income level and psychological states such as depression have been shown to be associated with physical function [9, 10], yet their combined influence on HGS in the Korean context warrants further investigation.
Given the rapid aging of the Korean population, there is a continuous need for up-to-date, nationally representative data to understand the current determinants of functional health. While previous studies have explored factors related to HGS, utilizing the most recent data allows for the identification of contemporary risk profiles and informs timely public health interventions. The Korea National Health and Nutrition Examination Survey (KNHANES) provides a comprehensive, high-quality dataset ideal for such an investigation, containing detailed information on sociodemographic, health, and nutritional variables from a representative sample of the nation.
Therefore, the primary objective of this study was to identify a comprehensive range of sociodemographic and health-related factors associated with HGS among community-dwelling older adults in Korea. By analyzing data from the 9th KNHANES (2022), this research aims to provide current, evidence-based insights that can help guide strategies for maintaining muscle strength and promoting healthy aging.
Methods
1. Study Design
This study utilized a descriptive, cross-sectional design to analyze secondary data from the 9th KNHANES, conducted in 2022. The primary objective was to identify various factors associated with handgrip strength in older adults residing in the community.
2. Data Source and Participants
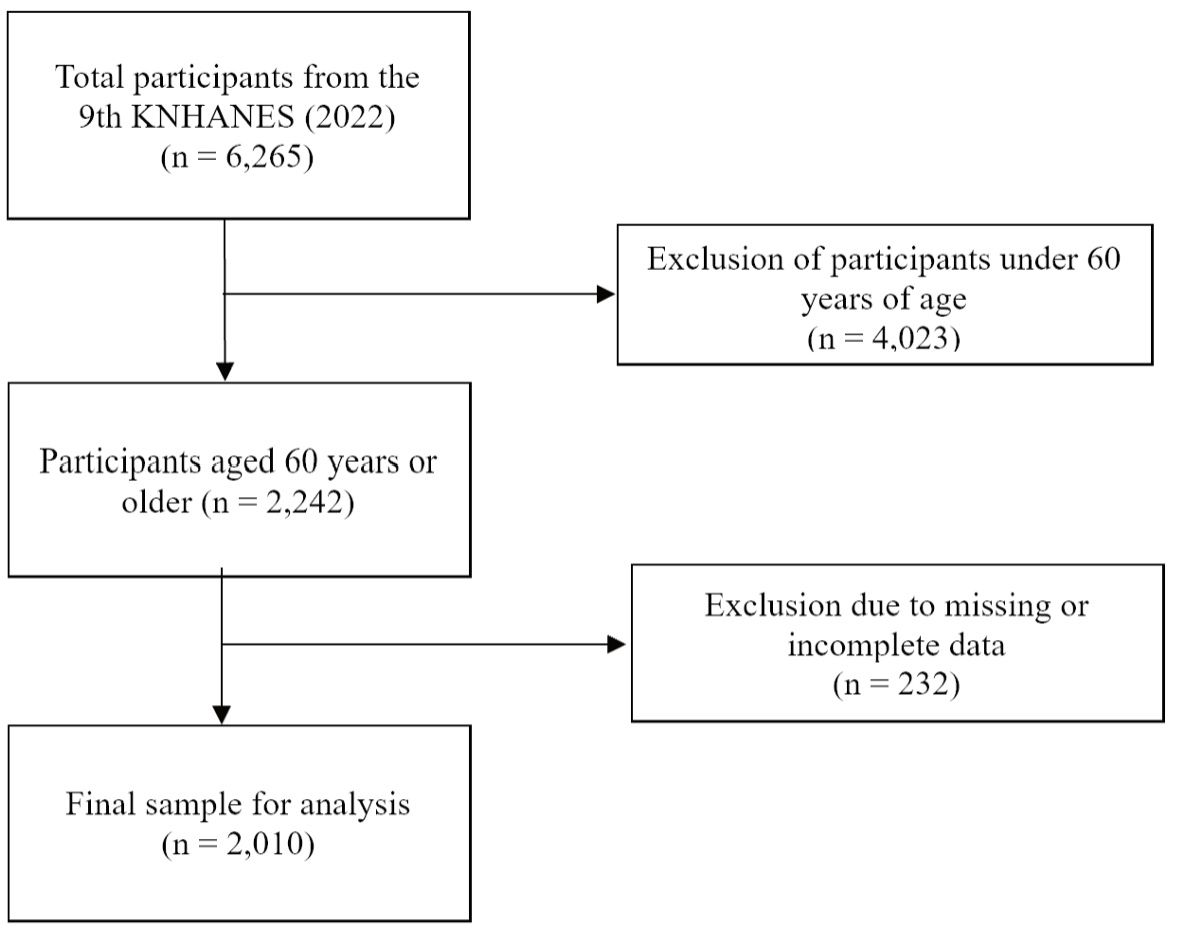
The initial dataset from the 2022 KNHANES included 6,265 individuals. For the purpose of this study, the sample was first limited to participants aged 60 years or older. This age threshold is a widely accepted criterion for defining older adults in gerontological research and aligns with definitions used by major health organizations such as the World Health Organization (WHO), as significant changes in physical function and muscle strength become more prominent from this age onwards [11]. This initial selection resulted in a pool of 2,242 potential subjects. From this group, 232 participants were subsequently excluded due to incomplete information about key variables, such as HGS. Therefore, the final analysis was performed on a sample of 2,010 older adults (Figure 1).
3. Measures
1) Dependent Variable: Handgrip Strength (HGS)
The primary outcome of this study was handgrip strength (HGS). It was measured using a digital grip strength dynamometer (T.K.K 5401, Japan), which records gripping force in a range of 5 to 100 kg with a precision of 0.1 kg. Following the KNHANES protocol, participants performed the test twice with their dominant hand, and the maximum value of the two measurements was used for the analysis. For the logistic regression analysis, HGS was categorized as a binary variable ("low HGS" vs. "normal HGS"). The classification was based on the cutoff points recommended by the Asian Working Group for Sarcopenia (AWGS): <28 kg for men and <18 kg for women were defined as low HGS [8]. Individuals with conditions that could interfere with an accurate measurement, such as hand or finger deformities, fractures, paralysis, recent wrist/hand surgery (within the last 3 months), or significant pain, were excluded from the HGS assessment.
2) Independent Variables
(1) Sociodemographic Characteristics
Sociodemographic factors were extracted from the KNHANES survey, including age (as a continuous variable) and sex (male or female). Educational attainment was categorized into four groups: elementary school or less, middle school, high school, and college or higher. Household income was calculated as the monthly household income adjusted for the number of family members and was subsequently divided into quartiles. Furthermore, marital status was dichotomized into two groups: "married and living with a spouse" and "widowed, divorced, separated, or never married."
3) Health-Related Characteristics
(1) Sociodemographic Characteristics
Sociodemographic factors were extracted from the KNHANES survey, including age (as a continuous variable) and sex (male or female). Educational attainment was categorized into four groups: elementary school or less, middle school, high school, and college or higher. Household income was calculated as the monthly household income adjusted for the number of family members and was subsequently divided into quartiles. Furthermore, marital status was dichotomized into two groups: "married and living with a spouse" and "widowed, divorced, separated, or never married."
(2) Health-Related Characteristics
Health-related variables included smoking status, alcohol consumption, physical activity, sleep duration, Body Mass Index (BMI), depression, and muscle mass. Smoking status was classified as "never," "former," or "current" smoker, while alcohol consumption was defined as drinking at least once a month over the past year. Physical activity was defined as engaging in at least 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic activity per week. Sleep duration was recorded as the average hours of sleep per day on weekdays. BMI was calculated as weight in kilograms divided by the square of height in meters (kg/m²) and was categorized into six groups: underweight (<18.5), normal (18.5–22.9), pre-obese (23.0–24.9), obese class I (25.0–29.9), obese class II (30.0–34.9), and obese class III (≥35.0) [12]. Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9), a 9-item tool evaluating symptoms over the past two weeks, with scores ranging from 0 to 27; a score of 10 or higher indicated depression [13], and the scale's Cronbach’s α in this study was 0.79. Lastly, muscle mass was measured using bioelectrical impedance analysis (BIA) with an Inbody 970 device. Low muscle mass was defined based on the appendicular skeletal muscle mass (ASM) divided by height squared (ASM/height²), using thresholds of <7.0 kg/m² for men and <5.7 kg/m² for women, consistent with the AWGS 2019 consensus [8].
4. Data Collection Procedure
This study utilized data from the 9th KNHANES, a nationwide, ongoing surveillance system designed to produce representative statistics on the health and nutritional status of the Korean population. The 2022 dataset was compiled from January to December, using a complex, multi-stage probability sampling method based on 25 households from 192 distinct regions across the country. A professionally trained team conducted the data collection through direct interviews and self-administered questionnaires [14]. For this secondary analysis, the raw dataset was formally obtained from the official KNHANES website after completing the required user agreements and security protocols.
5. Statistical Analysis
To ensure the findings were representative of the Korean older adult population, all analyses were conducted using the complex samples module of SPSS version 28.0, which accounts for the survey's intricate design by incorporating strata, clusters, and weight variables. Initially, descriptive statistics were used to summarize the participants' general and health-related characteristics. Categorical variables were presented as unweighted frequencies (n) and weighted percentages (%), while continuous variables were reported as means and standard errors. Subsequently, complex samples general linear model (GLM) was employed for univariate analysis to examine differences in participant characteristics according to their handgrip strength status. To identify the factors independently associated with handgrip strength in older adults, a multivariable logistic regression analysis was performed. The results of this analysis were presented as odds ratios (ORs) with their corresponding 95% confidence intervals (CIs). For all statistical tests, a p-value of less than 0.05 was considered to indicate statistical significance.
6. Ethical Considerations
The KNHANES protocol was formally approved by the Institutional Review Board of the Korea Disease Control and Prevention Agency (KCDA) (IRB No. 2018-01-03-4C-A). All individuals who participated in the survey provided written informed consent prior to their involvement. The dataset provided for public use was fully anonymized and de-identified by the KCDA to protect participant confidentiality in accordance with national privacy laws. As this study was a secondary analysis of publicly available and deidentified data, it was exempt from requiring separate institutional review board approval.
Results
1. Participant Characteristics
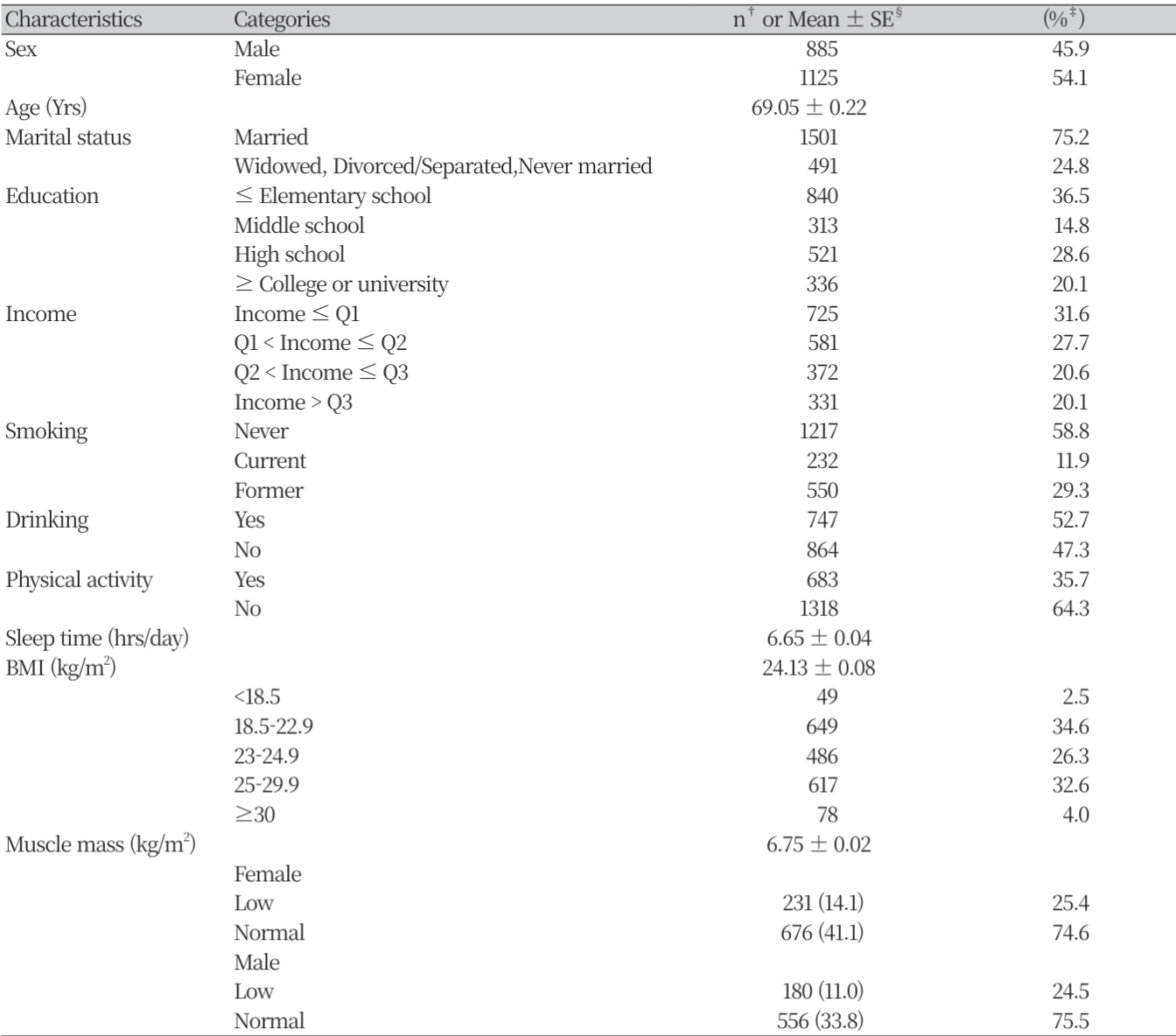
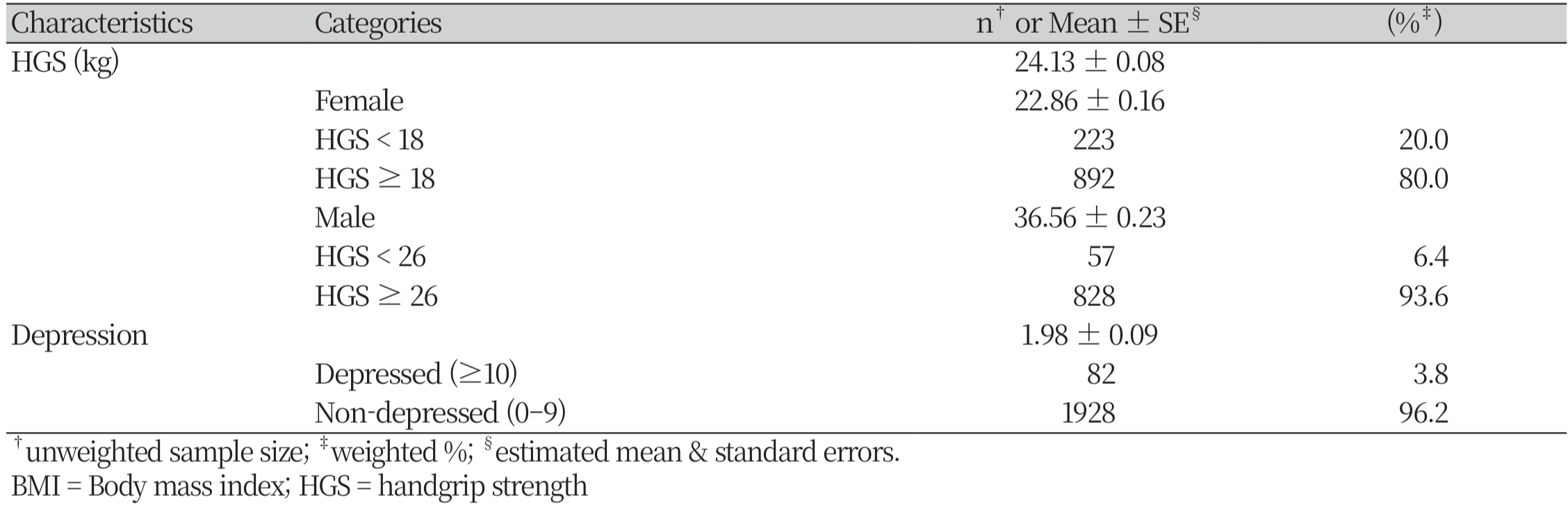
The sociodemographic and health-related characteristics of the 2,010 study participants are detailed in Table 1. Of the total participants, 54.1% were female, and the mean age of the study population was 69.05 ± 0.22 years. The majority of participants were married (75.2%). In terms of educational attainment, the largest proportion of participants had completed elementary school or less (36.5%), followed by high school (28.6%). For household income, the lowest quartile (Q1) was the most represented group, accounting for 31.6% of the sample. Regarding health-related factors, a majority of the participants were never-smokers (58.8%). Over half reported consuming alcohol (52.7%), while a significant portion (64.3%) did not meet the recommended guidelines for physical activity. The average sleep duration was 6.65 ± 0.04 hours per day. Based on Body Mass Index (BMI), 34.6% of participants were within the normal range (18.5–22.9 kg/m²), and 32.6% were in the obese class I category (25–29.9 kg/m²). The mean muscle mass for the sample was 6.75 ± 0.02 kg/m². When this was analyzed by sex, 24.5% of males and 25.4% of females were classified as having low muscle mass. The mean handgrip strength (HGS) for the entire sample was 24.13 ± 0.08 kg. When disaggregated by sex, the mean HGS was 36.56 ± 0.23 kg for males and 22.86 ± 0.16 kg for females. Based on the specific cutoffs for low HGS, 6.4% of males and 20.0% of females were classified into the low HGS group. Finally, the overall prevalence of depression in the study population was 3.8%.
2. Differences in Characteristics by HGS Group
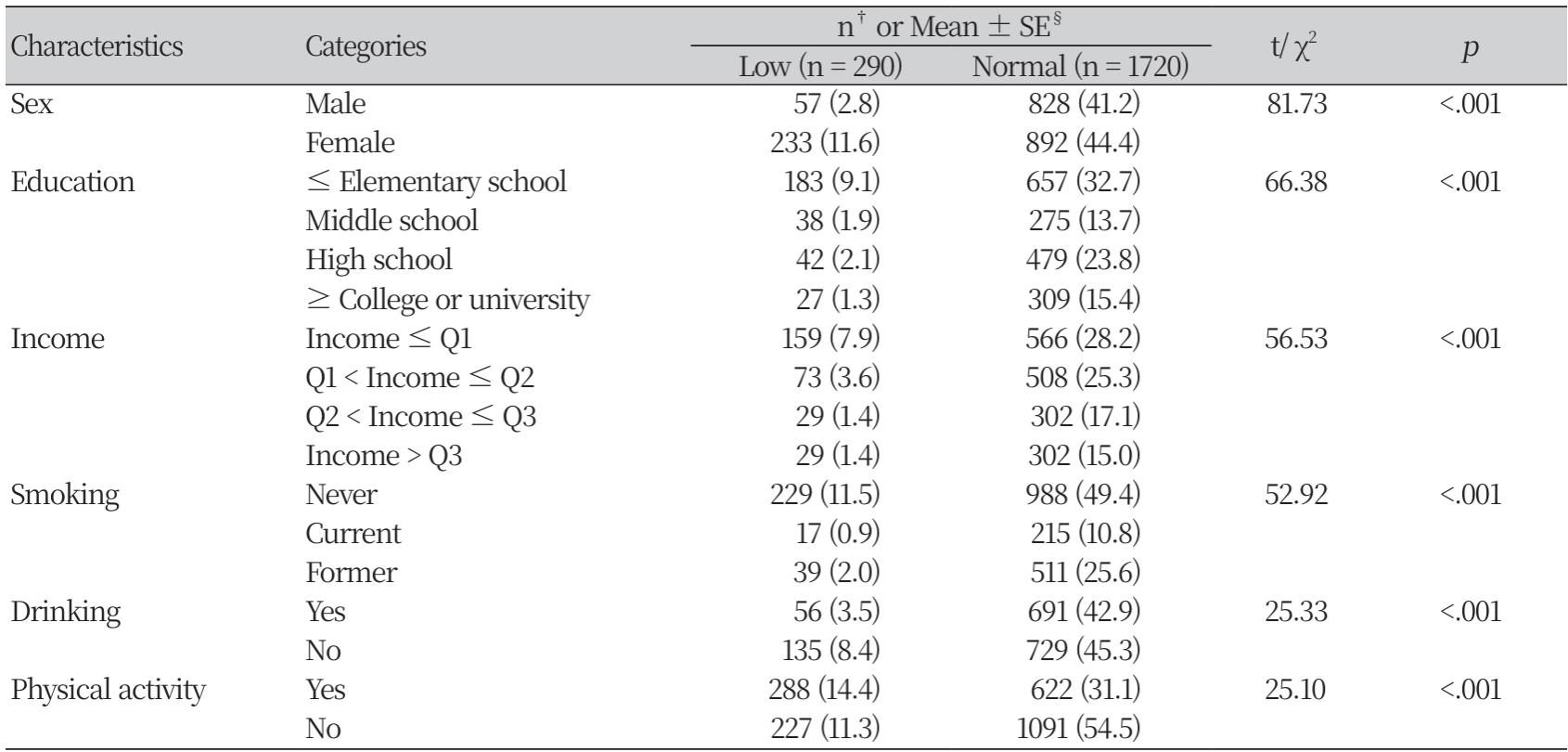
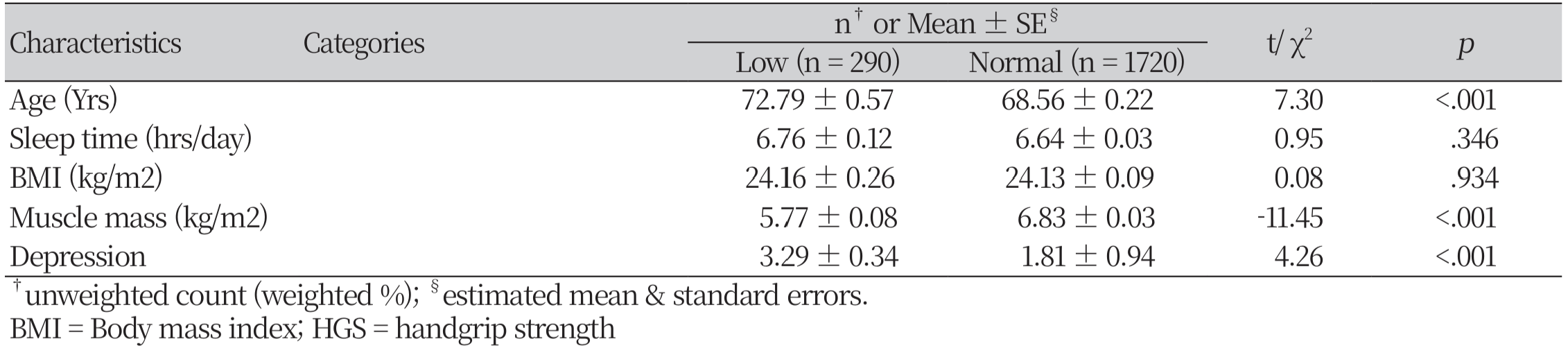
The comparison of characteristics between the low and normal handgrip strength (HGS) groups is presented in Table 2. The analysis revealed statistically significant differences between the two groups across most sociodemographic and health-related variables. Specifically, the low HGS group was significantly older (mean age 72.79 vs. 68.56 years, p<.001), had lower muscle mass (mean 5.77 vs. 6.83 kg/m², p<.001), and reported higher depression scores (mean 3.29 vs. 1.81, p<.001) compared to the normal HGS group. Furthermore, there were significant differences in the distribution of categorical variables. A significantly higher proportion of females was observed in the low HGS group (p<.001). Individuals in the low HGS group were also more likely to have a lower education level (elementary school or less) and belong to the lowest income quartile. Regarding health behaviors, the low HGS group was less likely to engage in regular physical activity and less likely to consume alcohol compared to the normal HGS group. In contrast, no statistically significant differences were observed between the low and normal HGS groups for mean sleep time (p=.346) or BMI (p=.934).
3. Factors Associated with HGS
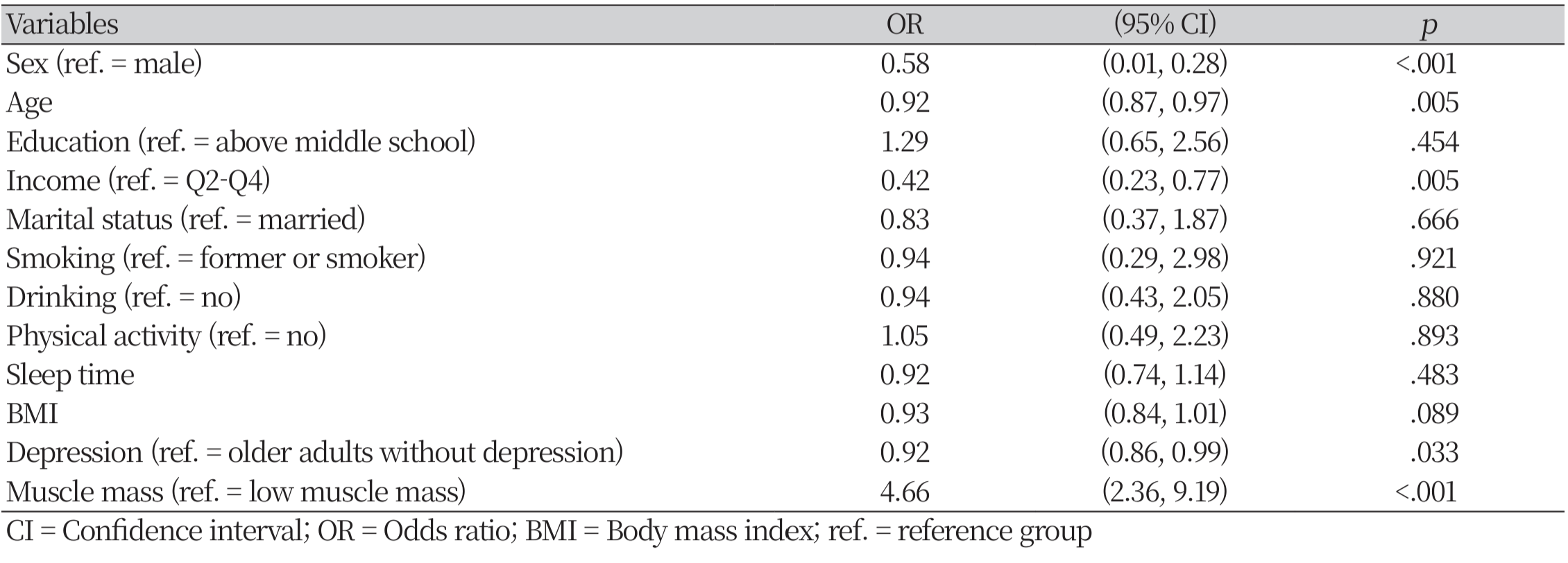
The results of the multivariable logistic regression analysis, performed to identify factors independently associated with having normal handgrip strength (HGS), are presented in Table 3. The most powerful factor associated with HGS was muscle mass. Participants with normal muscle mass had 4.66 times the odds of having normal HGS compared to those with low muscle mass (OR = 4.66, 95% CI [2.36, 9.19], p < .001).
Several sociodemographic factors were also significant. Females were less likely to have normal HGS than males (OR = 0.58, 95% CI [0.01, 0.28], p < .001). Each one-year increase in age was associated with an 8% decrease in the odds of having normal HGS (OR = 0.92, 95% CI [0.87, 0.97], p = .005). Furthermore, participants in the lowest income quartile had significantly lower odds of having normal HGS compared to those in higher income quartiles (OR = 0.42, 95% CI [0.23, 0.77], p = .005). Depression was also a significant predictor; higher levels of depression were associated with lower odds of having normal HGS (OR = 0.92, 95% CI [0.86, 0.99], p = .033). In contrast, education level, marital status, smoking, drinking, physical activity, sleep time, and BMI were not found to be statistically significant factors associated with HGS in the model.
Discussion
This study aimed to identify a comprehensive range of factors associated with HGS among community-dwelling older adults in Korea, using recent, nationally representative data from the 2022 KNHANES. Our findings revealed that having normal muscle mass was the most powerful determinant of normal HGS. Additionally, being male, younger, having a higher income, and exhibiting fewer depressive symptoms were all independently associated with higher odds of maintaining normal HGS. These results underscore the multifactorial nature of muscle strength in the aging population, involving physiological, demographic, socioeconomic, and psychological dimensions.
A key finding from this study is the robust and independent association between muscle mass and HGS, which, while anticipated, highlights the critical link between muscle quantity and function. As HGS is a direct measure of muscle function, its intrinsic link to the quantity of underlying muscle mass is physiologically coherent. This result aligns with the foundational principles of sarcopenia diagnosis, which defines the condition through a combination of low muscle mass and poor physical function (i.e., low HGS) [8, 15]. Similarly, the findings that HGS declines with increasing age and is lower in females are consistent with a vast body of existing literature, reflecting fundamental biological and hormonal differences [16].
Beyond physiological and demographic factors, our study reinforces the significant role of socioeconomic status and mental health in physical function. The finding that lower income was associated with lower odds of normal HGS suggests that socioeconomic disparities may manifest physically. Potential pathways could include differences in nutrition, access to healthcare, and opportunities for physical engagement [17]. Furthermore, the association between depressive symptoms and lower HGS highlights a crucial psycho-physical connection [9]. This relationship may be bidirectional; depression can lead to physical inactivity and anorexia, thereby reducing muscle strength, while declining physical function can, in turn, exacerbate feelings of depression and hopelessness [17, 18].
The findings of this study have several important implications for nursing education, practice, and research. In nursing practice, community and primary care nurses are ideally positioned to implement routine HGS screening for older adults as a 'vital sign' of functional health. Given the strong associations found, nurses should be particularly vigilant with patients who are female, older, have a low income, or exhibit depressive symptoms. Early detection of low HGS can trigger timely referrals to physical therapists, dietitians, and social services, facilitating early and targeted interventions. For nursing education, curricula should incorporate HGS assessment into geriatric care modules, emphasizing not only the measurement technique but also its clinical significance in identifying at-risk individuals and understanding the multifactorial nature of its determinants.
In terms of future research, this study highlights several key directions. Nurse-led studies are urgently needed to design and test the efficacy of multi-component interventions—for example, programs combining resistance training, nutritional guidance, and depression screening—to improve HGS, particularly in vulnerable populations. Furthermore, while our study identifies strong associations, longitudinal studies are required to elucidate the causal pathways between variables like depression, income, and HGS decline. Finally, qualitative research could provide deeper insights into the lived experience of functional decline, which is essential for designing more patient-centered and effective interventions.
Several limitations of this study must be acknowledged. First, due to its cross-sectional design, we cannot establish causality between the identified factors and HGS. For example, it is unclear whether depression leads to lower HGS or if lower HGS contributes to the onset of depression. Second, some variables, such as physical activity and income, were based on self-report, which may be subject to recall or social desirability bias. Finally, while we controlled numerous variables, other potential confounders like nutritional intake, inflammatory markers, or social support systems were not included in the analysis, indicating a need for further research.
In conclusion, this study provides nationally representative evidence that handgrip strength in older Korean adults is determined by a combination of modifiable and non-modifiable factors, with muscle mass, income, and depression emerging as key predictors. Based on these findings, we recommend the integration of HGS screening into routine clinical practice and community health programs for older adults, paying special attention to those with low income or depressive symptoms. Furthermore, public health interventions must be multifaceted, combining resistance exercise and nutritional support to build muscle mass with accessible mental health services and policies that address socioeconomic barriers to health. Adopting such a holistic approach is essential for effectively preventing functional decline and promoting healthy aging in this rapidly growing population.
Conclusions
In this nationally representative study of community-dwelling older Korean adults, we confirmed that muscle mass, demographic factors (age and sex), socioeconomic status (income), and mental health (depression) are all significant and independent determinants of HGS. The findings highlight that while all these factors are important, maintaining adequate muscle mass is the most powerful predictor of normal HGS. Therefore, public health strategies aimed at preventing functional decline in the aging population should adopt a comprehensive approach that not only promotes muscle-strengthening activities but also addresses socioeconomic inequalities and integrates mental health support. These results reinforce the value of HGS as a key indicator of overall health in older adults and underscore the need for multifaceted interventions to support healthy aging.
